Want to create or adapt books like this? Learn more about how Pressbooks supports open publishing practices.
3 Chapter 3 Local Community Planning Committees (LEPC), Strategic National Stockpile, ESF 8
Local Emergency Planning Committees
Under the Emergency Planning and Community Right-to-Know Act (EPCRA), Local Emergency Planning Committees (LEPCs) must develop an emergency response plan, review the plan at least annually, and provide information about chemicals in the community to citizens. Plans are developed by LEPCs with stakeholder participation. There is one LEPC for each of the more than 3,000 designated local emergency planning districts. The LEPC membership must include (at a minimum):
Elected state and local officials
Police, fire, civil defense, and public health professionals
Environment, transportation, and hospital officials
Facility representatives
Representatives from community groups and the media
What are the required elements of a community emergency response plan?
Identification of facilities and transportation routes of extremely hazardous substances
Description of emergency response procedures, on and off site
Designation of a community coordinator and facility emergency coordinator(s) to implement the plan
Outline of emergency notification procedures
Description of how to determine the probable affected area and population by releases
Description of local emergency equipment and facilities and the persons responsible for them
Outline of evacuation plans
A training program for emergency responders (including schedules)
Methods and schedules for exercising emergency response plans
Ada County LEPC
This page provides information about the Ada County Local Emergency Planning Committee (LEPC). Meeting schedules, meeting minutes and other information may be found on this page. If you have a suggestion for an agenda item, or a question about the Ada County LEPC please send an email to Chairman Joe Lombardo (jlombardo@adacounty.id.gov). In the subject line put: LEPC.
The Local Emergency Planning Committee is a product of federal legislation passed by Congress after the disaster in Bhopal, India, where thousands of people died from an accident involving hazardous chemicals. To prevent similar accidents in our communities, in 1986 Congress passed the Emergency Planning and Community Right to Know Act (EPCRA), also known as SARA Title III. EPCRA established requirements for businesses, and for federal, state, and local governments regarding emergency planning, and community-right-to-know reporting for hazardous chemicals. This helps increase public awareness about the presence of chemicals in their communities and any releases of these chemicals into the environment. The State of Idaho also enacted the Hazardous Substance Emergency Response Act (Idaho Code: Title 39, Chapter 71).
LEPCs are the link between citizens, industry and the government. The membership comes from the local area and is familiar with factors that affect public safety, the environment, and the economy of the community. In Ada County the LEPC charter has been expanded beyond just chemical hazards to include information and discussion about emergency planning, training and exercising, for all hazards.[1]
History, Purpose and Basic Requirements of EPCRA
History
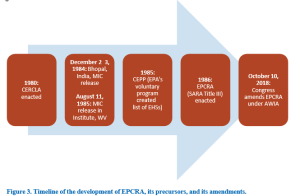
The Emergency Planning and Community Right-to-Know Act (EPCRA), also known as “SARA Title III,” was passed on October 17, 1986, in response to concerns regarding environmental and safety hazards posed by the storage and handling of hazardous chemicals. These concerns were triggered by two major chemical incidents.
Bhopal, India: December 1984
Late on December 2, 1984, a faulty valve at a Union Carbide facility allowed water to mix with a tank of methyl isocyanate (MIC), resulting in a vigorous exothermic reaction in the tank. At around 1:00 AM on December 3, a safety valve failed, releasing a plume of toxic gases, including MIC. By dawn, thousands of people were dead, along with buffaloes, cows, dogs and birds. Local hospitals were soon overwhelmed with the injured, a crisis further compounded by a lack of knowledge of exactly what gases were involved and what their effects were. Estimates of the number of people killed in the first few days by the plume run as high as 10,000, with 15,000 to 20,000 premature deaths reportedly occurring in the subsequent two decades. The government reported that more than half a million people were exposed to the gas.3
Institute, West Virginia: August 1985
Shortly after the Bhopal disaster, a chemical release from another Union Carbide facility further demonstrated that these types of incidents could happen anywhere and that many communities could be facing similar or worse catastrophic risks. A release of aldicarb oxime with other chemicals from this facility sent more than 125 people to the hospital and again highlighted the lack of information on industrial chemicals and their risks available to communities. This incident increased national attention to hazardous chemicals in
Figure 1. Front page of the New York Times, August 12, 1985, showing the Union Carbide incident in Institute, West Virginia.
The dual legislative purposes of EPCRA are reflected in its name: emergency planning and community right-to-know. The first part of the law requires facilities to report the presence and release of hazardous chemicals to federal, state, tribal and local authorities. The second part of the law is community right-to-know provisions, which require facilities to report inventories of hazardous chemicals and releases of toxic chemicals.
Basic Requirements of EPCRA Congress enacted EPCRA to establish requirements for federal, state, tribal and local governments and industry regarding emergency planning and release notification, community right-to-know, and reporting on hazardous and toxic chemicals. These requirements are essential to meeting EPCRA’s goal of improving local emergency preparedness and increasing community awareness of chemical hazards.
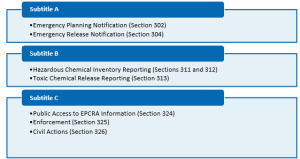
EPCRA has four provisions related to preparing the community for chemical accident releases, divided into Subtitles A and B:
· Subtitle A: Establishing the framework for state, tribal and local emergency planning.
○ Emergency Planning Notification (Section 302)
○ Emergency Release Notification (Section 304)
· Subtitle B: Mechanism for informing the public of the presence of chemicals and releases of toxic chemicals
○ Hazardous Chemical Inventory Reporting (Sections 311 and 312)
○ Toxic Chemical Release Reporting (Section 313)
Subtitle C contains provisions related to providing public access to EPCRA information, enforcement, and civil actions for failure to comply with requirements of EPCRA (Sections 324 to 326).
4 Environ Health. 2005;4(1):6. Published 2005 May 10. doi:10.1186/1476-069X-4-6; Sharma DC. Bhopal: 20 Years On. Lancet. 2005; 365:111–112. DOI: 10.1016/S0140-6736(05)17722-8.
Figure 2. EPCRA provisions.
Precursors to EPCRA Prior to EPCRA, federal, state and local programs assumed the responsibility for responding to chemical incidents. Emergency response was delegated to the National Response Team (NRT),5 Regional Response Teams (RRTs), and state and local response teams. A few of these programs are discussed below.
Figure 3. Timeline of the development of EPCRA, its precursors, and its amendments.
Comprehensive Environmental Response, Compensation, and Liability Act (CERCLA)The Comprehensive Environmental Response, Compensation, and Liability Act of 1980— otherwise known as CERCLA or Superfund—provides a federal “superfund” to clean up uncontrolled or abandoned hazardous-waste sites as well as accidents, spills, and other emergency releases of pollutants and contaminants into the environment. Through CERCLA,
5 The NRT is composed of representatives of 15 federal agencies with responsibilities for emergency preparedness and response. EPA and the U.S. Coast Guard (USCG) serve as Chair and Vice Chair, respectively. The National Oil and Hazardous Substances Pollution Contingency Plan (NCP) and the Code of Federal Regulations (40 CFR part 300) outline the role of the NRT and RRTs. RRTs consist of regional representatives of the federal agencies on the NRT, as well as state emergency response and preparedness officials.
EPA has authority to seek out those parties responsible for any releases and assure their cooperation in the cleanup.
EPA cleans up sites even if potentially responsible parties cannot be identified or located, or when they fail to act. Through various enforcement tools, EPA obtains private party cleanup through orders, consent decrees, and other small party settlements. EPA also recovers costs from financially viable individuals and companies once a response action has been completed.
EPA is authorized to implement the Act in all U.S. states and territories. Superfund site identification, monitoring and response activities in states are coordinated through the state and tribal environmental protection or waste management agencies.
CERCLA was the first federal law designed to address the release of chemicals in the environment, prior to the enactment of EPCRA. However, CERCLA did not address chemical preparedness in local communities. For example, CERCLA did not account for:
· Identifying on-site chemical storage at facilities.
· Pre-planning at state, tribal, and local levels.
· Training local emergency and medical personnel to deal with incidents involving exposure to chemicals.
In addition, the public did not have access to chemical inventory information under CERCLA.
The Superfund Amendments and Reauthorization Act (SARA) of 1986 reauthorized CERCLA to continue cleanup activities around the country. Section 103(a) of CERCLA “as amended” requires that the person in charge of a vessel or facility immediately notify the National Response Center whenever a reportable quantity (RQ) or more of a CERCLA hazardous substance is released in any 24-hour period, unless the release is federally permitted. The purpose of this requirement is to notify federal government officials of potentially dangerous releases so that they can evaluate the need for a response action.
Voluntary Chemical Emergency Preparedness Programs Prior to EPCRA Prior to 1986, a mandatory national emergency response program and comprehensive state and local programs to address chemical accidents were lacking in communities throughout the country.
The Bhopal tragedy prompted the initiation of several programs; some were voluntary. A few are discussed below.
EPA’s Chemical Emergency Preparedness ProgramAlthough emergency response programs such as CERCLA were in existence to respond to releases of hazardous substances and oil, there was no federal mandate to plan and prepare the community for chemical accidents. The Bhopal, India, tragedy demonstrated that substances that are acutely toxic and have a high potential for becoming airborne posed a hazard to the community. In many cases, public health and the environment may be impacted before emergency response personnel arrive on the scene of a release. For these types of releases, comprehensive emergency planning to prepare for the possibility of a release is vital to effectively protect the public and the environment. To address this, in June 1985, EPA initiated the voluntary Chemical Emergency Preparedness Program (CEPP) as part of the Agency’s Air Toxics Strategy for addressing both continuing and accidental releases of toxic substances into the air.
This voluntary program’s goals were to:
Increase community awareness of chemical hazards.
Better coordinate federal activities.
Develop state and local response plans for dealing with chemical accidents.
Under CEPP, EPA developed a list of substances and guidance materials to help local communities focus their planning efforts. The list of chemicals developed under the CEPP program later became the list of extremely hazardous substances (EHSs) established under EPCRA Section 302, which will be discussed in Chapter 2.
Industry and State Programs
At the same time as EPA established the voluntary CEPP program, the Chemical Manufacturers Association (now known as the American Chemistry Council (ACC)) also set up a voluntary program called Community Awareness and Emergency Response (CAER) for member companies to become more involved in their local community by explaining their plant’s operations and participating in local emergency planning.
More than 30 states passed laws (some even before the Bhopal tragedy) giving workers and citizens access to information about hazardous substances in their workplaces and communities. Some of the state programs required reporting of toxic chemical releases and the presence of hazardous substances. A few required information to be available to the public.[2]
Note that for the purposes of orientation the page numbers are the actual pages numbers within the document and not the .pdf page numbers.
Review Page iii of the document for the introduction (.pdf page 5) (printed below)
Review Page xi of the document for the distribution list to see who are considered partners (.pdf page 13)(Printed below)
Review pages 1 -18 for introduction and concept behind the plan (.pdf pages 15-35)
Drafting Your Response
Next, prepare your forum post by creating a Google document. On your document, answer the following questions:
What is you initial impression of the plan?
What was your impression of the distribution list? Does it show how the community is to work together?
Do you see a similarity between the ICS structure and how the plan is laid out?
What was most interesting to you about the items listed on pages 1-18
Be sure to support your responses by referencing materials from this module. Also, once you have answered the questions, be sure to proofread what you wrote before you share it.
Discussing Your Work
Discussing Your Work
To discuss your findings, follow the steps below:
Step 01. After you have finished writing and proofreading your responses, click on the discussion board link below.
Step 02. In the Discussion Forum, create a new thread and title it using the following format: Yourname and the topic of the discussion board.
Step 03. In the Reply field of your post, copy and paste the text of your composition from the Document you created.
Step 04. Add bolding, underlining, or italics where necessary. Also, correct any spacing and other formatting issues. Make sure your post looks professional.
Step 05. If you need to upload a document or image you can do so by clicking on the Upload image (photo image button) or Upload document (Document button) in the text editor and locating and selecting your document from your computer.
Step 06. When you have completed proofreading, fixing your post formatting, and attaching your file, click on the Post Reply button.
Emergency Operations Plan Basic Plan County, Idaho Emergency Operations Plan–Basic Plan |Draft,December2018
Section iii
ABOUT THIS PLAN The Ada County Emergency Operations Plan (EOP) contains a set of guidelinesdeveloped to assist in emergency response efforts to disasters occurring within AdaCounty, Idaho. The plan was written in accordance with the Federal EmergencyManagement Agency’s (FEMA)Comprehensive Preparedness Guide 101: Developingand Maintaining Emergency Operations Plans Version 2.0.This EOP is intended tointegrate with EOPs written for all levels of government, including cities within AdaCounty, neighboring counties in the region, the State of Idaho, and the National ResponseFramework. The Ada County EOP was developed based on guidance from FEMA(including the National Incident Management System [NIMS]), as well as lessons learnedfrom disasters and emergencies that have threatened Ada County in the past.
This EOP is promulgated with the understanding that major emergencies and disasters areunique events that have the potential to present the community and response personnelwith extraordinary problems and challenges that cannot be adequately addressed withinthe routine operations of government. Because the size and scope of any imaginabledisaster is impossible to predict, the Ada County EOP focuses on a streamlined, all–hazards preparedness approach to contingency planning rather than outlining highlydetailed operational procedures.Ada County is the most densely populated county in the State of Idaho. However, evengiven its significant capabilities for emergency response, Ada County assigns primaryresponsibility for preparedness and response to the following entities, in the followingorder: (1) individuals; (2) families; (3) local jurisdictions; and (4) Ada County. While it isthe intent of Ada County to prepare for, respond to, and mitigate all types of emergenciesand disasters, the reality is that during a major disaster, individuals and families shouldbe prepared to care for themselves for at least the first 96 hours.
This EOP provides fundamental guidance for emergency responders from all agenciesassigned specific functional responsibilities within the response effort. The EOP is basedon the premise that agencies will respond within their current capabilities. When thosecapabilities are exhausted, additional capabilities will be requested through mutual aid organizations, state agencies, and finally federal agencies.The development of the EOP and appropriate standard operating procedures is an ongoingprocess requiring annual review, training, and exercises. Implementation of the EOP willrequire extensive cooperation, collaboration, and training with government and non-government entities that are partners in disaster planning and response. Continuedcooperation and assistance to implement this County EOP is essential to improve AdaCounty’s ability to protect its citizens.
Section xi DISTRIBUTION LIST The plan is distributed electronically to all jurisdictions, agencies, stake holders and officials listed below. It is available to the public online at: Ada County 911 Dispatch Ada County Highway District Ada Community Public Library Ada County Assessor Ada County Commissioners Ada County Coroner Ada County Development Services Ada County Fairgrounds Ada County Operations Ada County Paramedics Ada County Parks Ada County Prosecutor Ada County Sheriff American Red Cross Boise Airport Boise Building Department Boise City Councilperson Boise Fire Department Boise Mayor Boise Parks Department BoisePolice Department Boise Public Library Boise Public Works Boise Risk Management Boise State University Boise Water–Master Central District Health Department Community Planning Association Eagle Fire District Eagle Mayor Eagle Public Library Flood ControlDistrict #10 Garden City Mayor Garden City Police Department Garden City Public Library Garden City Public Works Department Health south Treasure Valley Hospital Idaho Office of Emergency Management Idaho Department of Water Resources Idaho StateCommunication Center Idaho Transportation Department Idaho Power Idaho State Police Kuna Fire District Kuna Mayor Kuna Public Library Meridian City Clerk Meridian Fire Department Meridian Mayor Meridian Police Department Meridian Public Library Meridian Public Works Micron National Weather Service North Ada County Fire & Rescue District Saint Alphonsus Regional Medical Center Saint Luke’s Regional Medical Center Star Fire District Star Mayor Star Public Library SUEZ US Bureau of Reclamation US Army Corpsof Engineers Valley Regional Transit Veterans Administration Medical Center Whitney Fire District
Strategic National Stockpile
With more than 250 civil servants, U.S. Public Health Service officers, and contractors, the Strategic National Stockpile is organized to support any public health threat. Stockpile staff represent a variety of specialties, including pharmacy, clinical care, emergency management, medical logistics and operations, quality control, public health, procurement and financial management, information technology, strategic planning, training, policy and communications. All work together to ensure the right resources are ready and can get to the right place at the right time.
Strategic National Stockpile (SNS) has large quantities of medicine and medical supplies to protect the American public if there is a public health emergency (terrorist attack, outbreak, earthquake) severe enough to cause local supplies to run out. Once Federal and local authorities agree that the SNS is needed, medicines will be delivered to any state in the U.S. in time for them to be effective. Each state has plans to receive and distribute SNS medicine and medical supplies to local communities as quickly as possible.
ASPR’s Strategic National Stockpile (SNS), in coordination with the Centers for Disease Control and Prevention, is deploying vaccines and treatments to a number of jurisdictions across the United States to support communities affected by monkeypox.
Vaccines
The SNS holds both JYNNEOS and ACAM2000 vaccines that could be used to protect people from monkeypox infections. ASPR’s Biomedical Advanced Research and Development Authority (BARDA) supported the development of JYNNEOS, which is approved by the U.S. Food and Drug Administration (FDA) to prevent both smallpox and monkeypox. ACAM2000®, which was developed with support from SNS, is FDA approved for smallpox but could also be used to vaccinate at-risk individuals under an appropriate regulatory mechanism outside its labeled indication. CDC currently has an expanded access Investigational New Drug protocol that allows its use for monkeypox.
JYNNEOS vaccine may be shipped either frozen or refrigerated and requires specific cold chain requirements for storage. The requirements for shipment and storage differ from the package insert. Before requesting product, read Bavarian Nordic’s letter on storage requirements for JYNNEOS vaccine and ensure you have a plan to meet these requirements.
CHEMPACKs are containers of nerve agent antidotes placed in secure locations in local jurisdictions around the country to allow rapid response to a chemical incident. These medications treat the symptoms of nerve agent exposure and can be used even when the actual agent is unknown.
Because these antidotes must be administered quickly, the CHEMPACK team maintains 1,960 containers strategically placed in more than 1,340 locations in the United States. More than 90 percent of the U.S. population is within 1 hour of a CHEMPACK location. Most are located in hospitals or fire stations selected by local authorities to support a rapid hazmat response and can be accessed quickly if hospitals or first responders need them.
Federal Medical Stations
Supporting Medical Equipment and Pharmaceutical Needs in Emergencies
Federal medical stations (FMS) are rapidly deployable caches managed by the Strategic National Stockpile (SNS) that contain beds, supplies, and medicines that can quickly turn a pre-identified building into a temporary medical shelter during a national emergency. The FMS can support healthcare systems anywhere in the United States.
FMS Capabilities By The Numbers
50–250
Primary or critical care patients can be treated at each Federal Medical Station
3 day supply
of pharmaceuticals, medical equipment, and supplies deployed with each Federal Medical Station
15,000–40,000
square feet needed to operate a Federal Medical Station
Each FMS comes with medical and pharmaceutical resources to sustain from 50 to 250 stable primary or chronic care patients requiring medical and nursing services. The quantities of supplies provided differ between the 50 and 250-bed FMS. However, each come with a three-day supply of pharmaceuticals, medical equipment, and medical-surgical and general supplies including enhanced care treatment beds, hospital adjustable exam beds, IV poles, pediatric/toddler cots, portable cribs or pack and plays, housekeeping items, nursing station supplies, and personal protective items [e.g., gloves, gowns]), and other equipment for general, special care, and other non-acute care.
Because the equipment and supply cache does not include tents, each FMS requires an appropriate space in which to operate. A 250-bed FMS requires roughly 40,000 square feet of open space, while a 50-bed FMS requires about 15,000 square feet. Wrap-around logistical services must also be coordinated and in place before an FMS can be operational. FMS are not mobile and are not easily relocated once established.
Personal Protective Equipment
Supporting the Needs of Public Health and Healthcare Partners in an Emergency
Healthcare workers rely on personal protective equipment (PPE) to safeguard themselves and their patients against the spread of COVID-19 and other infectious diseases. HHS/ASPR’s Strategic National Stockpile (SNS) is the nation’s largest repository of emergency medical supplies to ensure that healthcare workers are equipped with the PPE they need to slow the spread of infection. When states, tribal nations, large metropolitan areas and territories cannot meet their PPE needs from their own stockpiles or from the commercial market, they can request SNS assets.
The SNS has provided millions of masks, gloves, gowns, N-95 respirators, face shields and other necessary supplies to minimize risk to healthcare workers as they care for patients across the country. These supplies are effective and critically important tools to help combat the COVID-19 pandemic.
Replenishing the SNS
As ASPR continues to expand and restructure the SNS, it is careful not to disrupt the supply chain so commercial distributors can still fill orders from U.S. healthcare facilities to meet current needs.
The SNS has greatly increased N95 respirators and ventilators on hand since pre-pandemic inventory. Other critical personal protective equipment such as surgical masks, gowns, coveralls, eye protection and have been added to inventory.
SNS-Held Ventilator Resources
The Strategic National Stockpile (SNS) can provide a variety of ventilator models to supplement state and local supplies in an emergency, and each ventilator has different features and modes of ventilation.
Sustaining the Stockpile
Sustaining the Strategic National Stockpile (SNS) involves managing the entire life cycle of stockpile assets as well as acquiring, storing, and transporting supplies.
SNS management includes:
Overseeing the shelf life of medicines to ensure the stock is rotated and kept within U.S. Food and Drug Administration (FDA) potency shelf-life limits
Conducting routine quality assurance on all products
Performing annual inventory of all products
Inspecting environmental conditions, security, and package maintenance
Ensuring SNS holdings are based on the latest scientific data and threat levels
Ensuring the ability to transport items during a public health emergency
Shelf Life Extension Program
The SNS participates in the Federal Shelf Life Extension Program (for federal stockpiles) which is managed by the Department of Defense and the FDA. Once the FDA conducts stability testing and determines that products are stable and safe for continued use, the program will extend the use-by dates of pharmaceuticals beyond their original expiration dates. Testing typically provides an added 12 to 24 months of extended shelf life. More testing can lead to even longer extensions. Products that fail FDA testing are removed from stockpile inventory.
Participation in the Shelf Life Extension Program requires:
Tracking the expiration date and manufacturer lot numbers of eligible products
Coordinating the shipment of products to FDA for stability testing
Receiving and tracking FDA testing results for each lot of product
Disposing of and replacing product lots that have failed FDA testing
Inventory Management and Tracking System
In a large-scale public health crisis, state and local public health agencies will have to manage large quantities of medical countermeasures (MCMs) to help prevent or treat diseases. Responders need an effective software tool to manage the large and rapidly moving MCM inventory they may receive from the SNS.
The Inventory Management and Tracking System (IMATS) was created by the SNS to help state and local public health agencies manage these MCMs during a crisis. IMATS allows responders to track MCM inventory down to local levels; monitor reorder thresholds; and support warehouse operations. This tool can also be used in regular day-to-day operations.